Anaesthetic use in removing wisdom teeth
Introduction

If you go to the dentist and need your upper backmost wisdom teeth removed, the dentist will likely give you an injection in the gum and also an injection in the roof of your mouth. The injection in the roof of the mouth is called a palatal anaesthetic. It can be quite painful and can result in swelling and discomfort after the tooth is removed. Dr. Mark Badcock wondered if the palatal anaesthetic was really helping to reduce pain. His experience as a dentist suggested that it might not.
The key question Mark wanted to answer was:
Is palatal anaesthetic needed when removing the third upper molar teeth?
Timeline
- 2002
-
Idea to conduct an experimental trial to investigate clinical experience.
- September 2002
-
Ethics applications to The University of Melbourne’s Human Research Ethics Committee, and the Ethics in Clinical Research Committee of the Department of Human Services, State Government of Victoria.
- 2003
- March 2004
-
Participants recruited and data collection commences.
- January 2005
-
Data analysis commences.

Backgound
Anaesthetising the mouth when an upper back wisdom tooth needs to be removed involves two injections – one into the gum and one into the roof of the mouth. Although this is the currently accepted practice, there is little research evidence relating to the use of the palatal injection. The justification for using the palatal injection is based on the anatomy of the nerve supply to the mouth. The intention is to block the supply to the palatal nerve so that the rear part of the hard palate and the overlying soft tissues become numb. It is thought that this assists in anaesthetising the teeth.
The palatal lignocaine injection can be quite painful as the tissues in the palate are quite dense. There can also be side effects later on, when the roof of the mouth can feel swollen, making breathing and swallowing uncomfortable. Mark Badcock believed that patients would not experience a greater level of discomfort during extraction if they did not have the palatal lignocaine injection. And, he hoped that if the palatal lignocaine injection could be avoided, then the patient would not have to experience the pain of the injection itself.
In this double-blind randomised controlled trial, neither the surgeon nor the patient needed to know which side of the mouth would receive a palatal injection of lignocaine – the current standard of care. This also meant that the patients needed to receive two palatal injections – one with the active anaesthetic and one without. Hence, Mark was able to compare the levels of pain experienced with and without an active anaesthetic. Patients still experienced the pain of the palatal injection on both sides of the mouth.
Mark regarded the study design as a stringent test of his idea. He reasoned that the side getting no palatal lignocaine was still getting the pain of a physical injection (with no active anaesthetic). If this side experienced less pain, or “equivalent” pain to the standard care group, then Mark felt that he could be confident that giving no palatal injection at all would be even better.
Study design
Interventions
Lignocaine injection on one side of the mouth
Saline injection on the other side
Variables measured
Immediate post-surgery
Level of pain during surgery on each side
3 hours post-surgery
- Current level of pain on each side
- Patient’s guess of the side injected with lignocaine
- Most comfortable side in 3 hours post-surgery
Statistician’s description of the design
The study was a randomised controlled trial that compared the effects of lignocaine and saline injections on the level of pain reported during and after upper molar surgery. Patients acted as their own controls; each patient had upper molars on both sides removed, but received a different palatal injection on each side. The study was double blind as neither the dentist nor the patient knew which side received lignocaine.

Calculating the sample size for the study
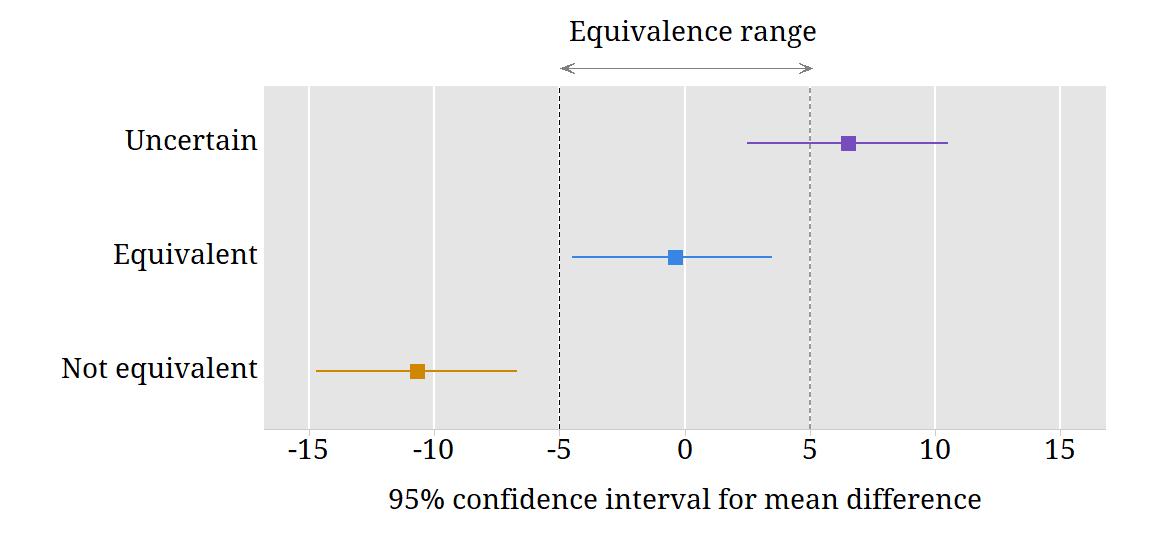
The study was an equivalence trial; the aim was to show that the average pain levels experienced with or without a palatal injection were equivalent. The differences between the treatments were expected to be small and must be estimated with good accuracy. The sample size calculations were based on a confidence interval for the mean difference between the two treatments.
“The relevance of the confidence interval … is easier to see. This defines a range for the possible true differences between the treatments, any point of which is reasonably compatible with the observed data. If every point within this range corresponds to a difference of no clinical importance, then the treatments may be considered to be equivalent.” (Jones, Jarvis, Lewis & Ebbutt, 1996).
An estimate of the sample size needed was calculated in the following way:
- The measurements of the level of pain from the Visual Analogue Scale were considered; the scores could range from 0 (no pain at all) to 100 (the worst pain imaginable).
- The differences between treatments on the Visual Analogue Scale were estimated to range between -30 and +30; this implies that the standard deviation of the differences is 10.
- The true mean difference between the treatments is assumed to be zero. An equivalence range for the mean difference between the treatments was defined as -5 to +5; in this range, the differences between the treatments are considered to be clinically negligible. The confidence interval should fall inside this range.
- The level of risk of the confidence interval falling wholly or partly outside the equivalence range was set at 0.2; hence, the long-term relative frequency of confidence intervals falling inside the equivalence range was 0.8.
- With the parameters described above:
- population standard deviation of differences = 10
- population mean difference = 0
- equivalence range -5 to +5
- 80% of confidence intervals falling inside the equivalence range in the long run
The sample size required was n = 42 patients.
This figure shows the equivalence range for differences between the saline and lignocaine injections. It also shows examples of confidence intervals for this difference. The width of the confidence interval is approximately 4 divided by the square root of the sample size.
Randomisation procedure
The planned 50 participants were randomly assigned to receive an injection of lignocaine on either the left side roof or the right side roof of their mouth, and a saline injection on the other side of the roof of their mouth. The random assignment was done in two blocks of 25 patients. Mark planned to analyse the data half way through the trial to see if the outcome was strong enough to stop the trial.
A computer-generated randomisation list was used. Mark Badcock who obtained the list from Randomization.com — a website that generates randomisation lists. The list was sent to the pharmacy staff who prepared the saline and lignocaine solutions for the palatal injections.
Double blinding
Mark Badcock performed all the surgery for the study. For each patient, two vials for the palatal injection were prepared under sterile conditions by the Clinical Trials Department at the Royal Melbourne Hospital Pharmacy. One contained saline and the other lignocaine. The paired vials were labelled “left” and “right” according to the randomisation assigned to that particular patient. When Mark operated on the patient, he did not know which side received lignocaine. The patient also did not know which vial contained lignocaine. However, it was possible that during the surgery, the patient may have become aware which side of the roof of his or her mouth felt numb and which did not. It was important that the patient did not tell Mark about this. Mark waited until after the surgery to get any information from the patients about the pain they experienced on both sides of their mouth.
Mark used a computer program to carry out the randomisation. The list of patient numbers and the side on which they received lignocaine was kept by staff in the Clinical Trials Department at the Royal Melbourne Hospital Pharmacy. Mark was only allowed to “break the code” to find out the randomisation at the end of the study, or in some special circumstances described below.
Procedures for meeting ethical concerns
Patients were being asked to undergo a potentially painful procedure without an anaesthetic injection to the roof of the mouth; a dentist would usually give this anaesthetic. A number of procedures were put in place to meet the ethical concerns raised by the study.
Patient withdrawal
Patients were told that they were able to withdraw from the study at any time.
Discontinuing the treatment
If a patient indicated that the pain level was too high, additional (lignocaine) anaesthetic was given, first in the gum and then in the palate if necessary.
Discontinuing the study
If, at any time, five patients required an additional palatal anaesthetic, the allocation of treatments to these patients was examined (before the trial ended). If all five additional palatal injections were on the saline side, the trial was to be stopped; if not, then treatment allocation was to be checked for each subsequent patient who needed an additional palatal injection. If, at any time, more than 10% of the patients treated to date needed an additional palatal injection on the saline side, the trial was to be stopped.
No one who came to the surgery withdrew from the study. No one needed additional palatal anaesthetic. The study was completed with full participation of all patients.
Mark analysed the data after treating 28 patients. The study was continued; the final sample was 51 patients.
Reference
Jones, B., Jarvis, P., Lewis, J.A., & Ebbutt, A.F. (1996). Trials to assess equivalence: the importance of rigorous methods. British Medical Journal, 313, 36-39.
Protocol
| Patient identification | Patients attending the Oral Surgery Department of the Royal Dental Hospital of Melbourne, requiring removal of both upper back wisdom teeth, are identified by independent clinicians who are not involved in the study. |
|---|---|
| Patient recruitment | Patients are invited to participate by a staff member from the Department of Oral Surgery and given a plain language explanation of the study. |
| Informed consent | If the patient agrees to participate, he or she is provided with Informed Consent form and ask to sign. An appointment was made for the surgery. |
| Assignment to the treatment side for lignocaine | The randomisation list is a list of patient numbers from 1 to 50 with the assignment of lignocaine to either the left or right side of the mouth. The vials containing the palatal injections are prepared for each patient according to the list by the Royal Melbourne Hospital Pharmacy. The first patient receives the first assignment on the list, the second patient receives the second, and so on. The surgeon opens the treatments prepared for the particular patient, but remains unaware which palatal injection if saline and which is lignocaine. The patient is injected with saline on one side of the palate and lignocaine on the other. |
| Surgical procedure | The surgeon waits for five minutes, and then removes the upper right side molar first, followed by the upper left side molar. Standard surgical procedures are followed. |
| Patient data collection – immediate | At the end of the surgery, patients are asked to rate their level of discomfort during the extraction using a visual analogue scale. The rate the side is extracted first, and then the side extracted second. |
| Patient data collection – 3 hours later | Patients are asked to take a form home to complete three hours after the surgery. On this form, the patients again rate pain on each side using a visual analogue scale, to indicate which side was more comfortable, and to guess which side received lignocaine. Patients were asked to return the form by post or to bring it to their follow-up appointment. |
Measuring the VAS responses
The distance of the mark from the left end of the scale was measured; the maximum was 135mm. The data have been rescaled so that the minimum (no pain at all) was 0 and the maximum was 100.

The figure shows the Visual Analogue Scale for rating pain. Patients placed a mark on the scale to indicate the level of pain experienced.
Summary
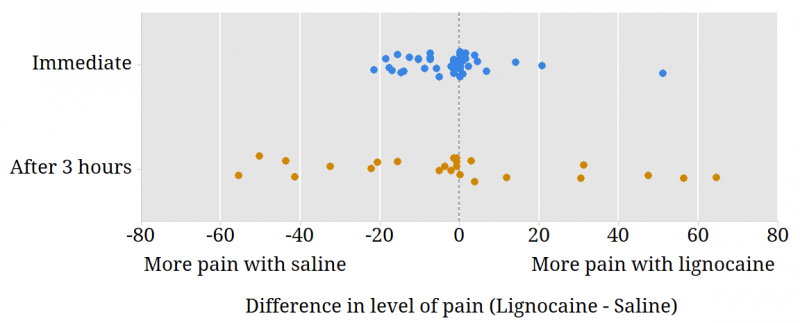
Fifty-one people participated in the study and all provided ratings of the pain experienced during the extraction. However, pain ratings 3 hours after surgery were only collected from patients in the first half of the trial; data were available for 25 patients.
There was a tendency for people to experience more pain on the saline side during extraction. Three hours after surgery, the differences in the pain experienced were highly variable; some people had more pain on the lignocaine side and others had more pain on the saline side. This can be seen in the figure above.
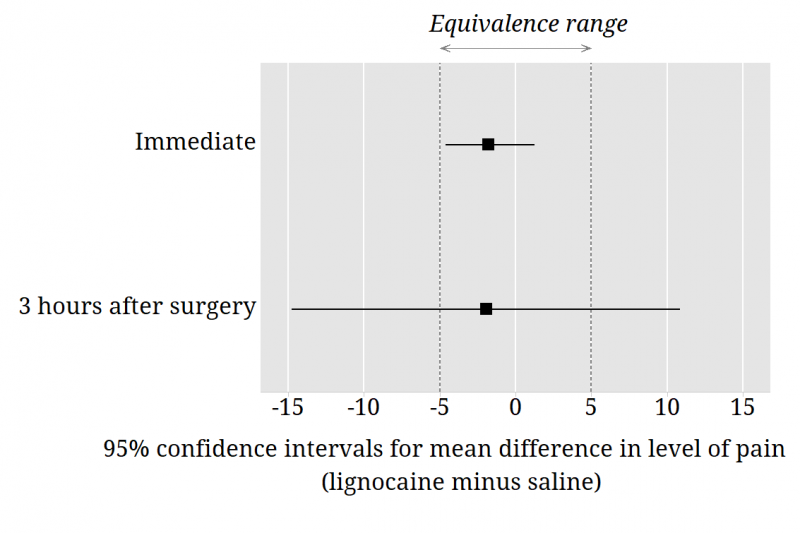
The wide 95% confidence interval for the mean difference in the level of pain experienced after 3 hours means that estimation of this difference is imprecise. The confidence interval is wide because there was large variability in the differences in the pain ratings after 3 hours and also because there were only 25 patients who provided the 3-hour ratings.
The confidence interval for the difference in pain rating during extraction is inside the equivalence range; we can consider the treatments to be equivalent. This confidence interval was obtained using bootstrap methods.
Questions to consider
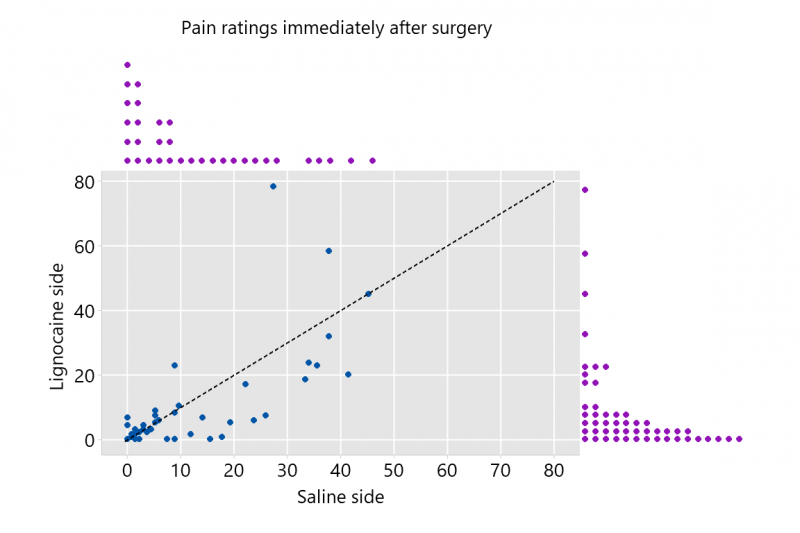
- The marginal plot to the left shows the ratings of pain on each side immediately after surgery. The dotted black line on the plot is the line y = x. Write an explanation of what the plot shows that could be understood by someone who is unfamiliar with statistics.
- Examine the differences in the pain reported under different treatments during surgery. Describe the features of the data.
- Consider the hypothesis that there is no difference in the pain reported under different treatments during surgery. Investigate different procedures for examining this hypothesis. Given the characteristics of the data, which approach would you recommend?
- Describe the differences in the pain reported under different treatments 3 hours post-surgery.
- Find a 95% confidence interval for the difference in reported pain under the two treatments 3 hours post-surgery. Describe the differences in the level of pain that patients report.
- Consider the patients’ guesses of what was injected in the lignocaine side. Find a 95% confidence interval for the proportion correct. Describe the accuracy of the patients guesses. Examine both the immediate and 3 hours post-surgery guesses.
- Investigate the relationship between the side receiving lignocaine and the side considered more comfortable during the 3 hours post-surgery.
- Consider the main outcomes for the study. What do the data suggest about Mark Badcock’s idea?
Definition of variables in data file
| Side receiving Lignocaine | Side of mouth receiving lignocaine treatment |
|---|---|
| VAS lignocaine during extraction | Visual analogue score for the lignocaine side during extraction |
| VAS lignocaine 3 hours later | Visual analogue score for the lignocaine side 3 hours after surgery |
| VAS saline during extraction | Visual analogue score for the saline side during extraction |
| VAS saline 3 hours later | Visual analogue score for the saline side 3 hours after surgery |
| More comfortable side | More comfortable side during 3 hours after surgery |
| Guess lignocaine side immediate | Patient’s guess of what was injected in the lignocaine side (immediate post-surgery) |
| Guess lignocaine side 3 hours later | Patient’s guess of what was injected in the lignocaine side (3 hours post-surgery) |
Glossary
Bootstrapping
A statistical technique used to estimate the sampling distribution of an estimator by resampling the data a large number of times.
Lignocaine
A local anaesthetic that is easily absorbed when injected into muscle.
Palatal anaesthetic
An injection of lignocaine into the roof of the mouth that makes the roof of the mouth numb.
Saline
A salt and water solution.
Third upper molar
The molars are the back-most teeth in your mouth. They are often called wisdom teeth. People typically have three molars on each side of the mouth, both at the top and at the bottom. The third upper molars are (usually) the back-most top teeth.