Health risks of fire-fighters
Introduction
There are very few occupations in the Western world today that involve serious health risks. Fire-fighters' work can, at times, involve exposure to hazardous situations, and materials and substances. For over 100 years, epidemiologists around the world have studied the health of fire-fighters. Interpretation of the outcomes of many studies can be tricky, but there are statistical methods for combining the results of many studies together.
The Metropolitan Fire and Emergency Services Board (MFESB) in Victoria, Australia wanted to know what the combined research evidence was for the risk of cancer and heart disease in fire-fighters. The key question was:
- What is the cumulative evidence of the health risks of being a fire-fighter compared with the general population?
Timeline
- July 2002
-
MFESB commissions a systematic review of epidemiological studies of fire-fighters; the Study design is discussed. - August 2002
-
Data collection commences by collecting published research and through literature searches. - October 2002
-
Study authors and researchers emailed to enquire about studies of fire-fighters known to them; 23 of the final 30 studies had been identified.
- 2002 - 2003
-
All studies to be included in the meta-analysis identified, and Data analysis commences.
- June 2003
-
Report to the MFESB.
The hazards of fire fighting
The possible occupational hazards associated with the profession of fire fighting have been studied for many decades. Firefighters may be exposed to the direct risk of injury or death from fire. The nature of the modern fire fighter’s work involves occasional exposures that are avoided by design in almost all other industries where they may have present in the past. Of course, similar minimization of exposure is attempted in the fire fighting industry also, but the unpredictability of fire means that prevention of hazardous exposure cannot be guaranteed in all circumstances.
Fires emit hot air and smoke, and in modern times the components of the smoke emitted from fires may involve complex chemical compounds, which in some circumstances could be carcinogenic. The inhalation of hot air, and products of the combustion of such substances as commonly-used plastics can be directly harmful to the lungs. However, even when an acute pulmonary injury is avoided, there may be subtle adverse effects on the health of exposed workers, which may manifest in a long-term outcome, possibly one removed in time from the key periods of exposure.
In addition to these prima facie considerations of exposures and possible hazards, the occupation of fire fighting, particularly in an urban context, appears to unusually well-documented. In many Western countries, there have been thorough and well-preserved historical records of the employment and health history of urban fire fighters, perhaps because they are operating in a risky profession on behalf of the rest of the community. There cannot be too many professions that can claim a “card index” of employment records dating back to 1869, as is the case for the Boston Fire Department (Musk et al, 1978).
For all of these reasons, the occupation of fire fighting has received considerable attention in occupational epidemiology. Many large studies have been carried out in communities in several continents. These studies have yielded results that are not entirely consistent. A number of reviews have been carried out, in an attempt to summarize the findings of the studies.
The need for meta-analysis
The Metropolitan Fire and Emergency Services Board (MFESB) in Victoria, Australia recognised the need for an up-to-date analysis of the combined research evidence for the risk of cancer and heart disease in fire-fighters.
You can see the list of studies included in the meta-analysis in the accordion below, and you can find the complete references with further details in the Glossary.
-
Study ID Name of study First author S001 Philadelphia fire fighters cohort study Baris S002 Death certificate study of US fire fighters, race and cancer mortality Ma S003 San Francisco fire fighters study Beaumont S004 Boston fire fighters study Musk S005 New Zealand fire fighters study Bates M S006 Western Australia fire fighters study Eliopulos S007 Second Toronto fire fighters study Aronson S008 Stockholm fire fighters study Tornling S009 Northwestern US states fire fighters study Demers S010 Melbourne fire fighters study Giles S011 Paris fire fighters study Deschamps S012 Buffalo fire fighters study Vena S013 Danish fire fighters study Hansen S014 Alberta urban fire fighters study Guidotti S015 New Jersey mortality study Feuer S016 Missouri case-control study Brownson S017 First Toronto firemen study Mastromatteo S018 Massachusetts fire fighters study Sama S019 Boston Normative Aging Study Dibbs S020 Washington brain tumour case-control study Demers S021 Toronto firemen coronary artery disease study Bates J S022 27 state PMR study Burnett S023 Seattle and Tacoma fire fighters cancer incidence study Demers S024 Canadian labor force mortality study Howe S025 Honolulu fire fighters study Grimes S026 Great Britain fire fighters study Gooderson S027 Connecticut fire fighters heart disease study Sardinas S028 California fire fighters study Cal DHS S029 Florida fire fighters study Ma S030 Massachusetts occupational study Dubrow
Study design
Inclusion criteria
Case-control studies, cohort studies and proportional mortality studies were included in the meta-analyses. The studies could be from any country, but must be reported in English. Unpublished and published research was eligible. The study needed to include fire-fighters as an occupational group by definition, but might also include other occupational groups.
Searching for the studies
- Provision of references and articles known to the MFESB.
- Internet and library database searches for other studies not included in the MFESB literature; a core list of studies was identified from the MFESB literature and the searches.
- Emailing lead authors of studies on the core list to ask about any studies that might not be included in the core list.
Extracting the data
In most cases, data were extracted from research publications. In one case (study 028), the publication was not available; however the data were included in a report of another study. Study 026 was found reported on a government web-site, but was not reported in an academic forum or publication. Attempts to contact the study author at the time were unsuccessful so the data were extracted from the website.
The statistician reviewed publications for each study and recorded details of each study on a data sheet. This included information about the study location, duration, reference populations and design. Statistical results were also recorded.
Obtaining the estimates and standard errors
The data needed for meta-analysis include an estimate of the relative mortality (or incidence) for fire-fighters, along with a standard error. For all studies, an estimate was available from the published reports. In all appropriate cases, the observed number of deaths (or cases) was reported. However standard errors were not uniformly reported. Some studies reported the expected number of deaths (or cases), some studies provided standard errors, and other studies reported confidence intervals for the estimate.
Summary
Thirty epidemiological studies provided substantial evidence about the health risks of being a fire fighter.
The studies were predominantly conducted in the USA, and included 23 in North America (19 in USA, four in Canada), 4 in Europe (Denmark, France, Sweden, UK) and 3 Australasian studies (2 in Australia, one in New Zealand).
In the 21 cohort studies alone, a total of hundreds of thousands of years of follow-up has been observed.
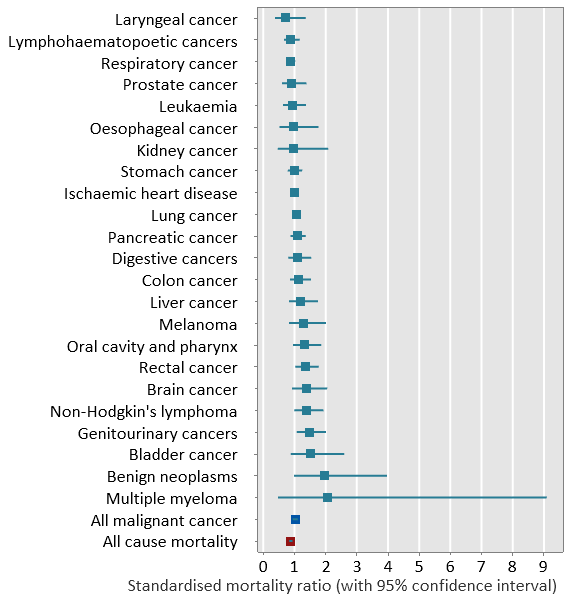
The figure shows the meta-estimates and 95% confidence intervals from the 21 cohort studies for 23 different individual cancers, ordered by the standardised mortality ratio.
It also shows the meta-analytic results for All malignant cancer and All cause mortality.
These analyses of the cohort studies used a random effects model.
Questions to consider
- Examine the figure on the Introduction page. You might consider combining the results from the 13 studies by taking an average of the 13 estimates. When might this strategy be appropriate? Are there any drawbacks of using this approach?
- Publication bias is often a concern in meta-analysis. What steps were taken to attempt to minimize publication bias in the meta-analyses considered here?
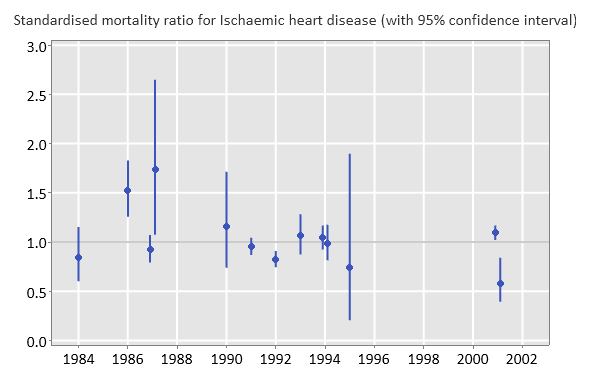
- Read the excerpts (in the accordion below) from publications of 13 studies of Ischaemic heart disease in firefighters that have been taken from the abstract, results and conclusions. How would you summarise this information? What conclusion about heart disease in fire-fighters might you draw after reviewing these excerpts? How valid do you think that conclusion is?
- Imagine you are a consultant advising a client. The client has taken excerpts (in the accordion below) from publications of 13 studies of Ischaemic heart disease in fire-fighters. She finds the results a little difficult to integrate. What would you suggest she do? Explain the advantages of your proposal.
- Consider working out a weighted average of the estimates from the 13 studies of Ischaemic heart disease in fire-fighters to obtain a single overall estimate. What features of the study might you consider in choosing the weights? Which studies should be given relatively greater weights? Propose a weighting that reflects this.
- Someone reviewing one of the papers is a little confused by the following extract: "Moreover, the confidence intervals for the overall age of 45 to 54 is such that the SMR is within the 95% confidence limits." Clarify the extract.
- Again imagine you are a consultant advising a client. The client has summarised the results from publications of 13 studies of Ischaemic heart disease in fire-fighters and shows you the table she produced. (See the accordion below.) Comment on the way she has summarised the results. What improvements would you suggest? Explain the advantages of your suggestions.
-
S006 - 1984
There was no evidence of increased mortality from cardiovascular or respiratory disease, or from any other cause.
There is virtually no evidence in these data of an adverse effect of fire fighting on mortality.
S027 -1986
Standardised mortality ...ratios for firemen and policemen are greater than 1.00.
Although some increased IHD risk for firemen and policemen is suggested, the exact role of occupational risk factors remains to be determined.
S012 - 1987
All diseases of the circulatory system including [ischaemic heart disease] ... did not differ significantly form the US general population, although ... slightly lower-than-expected heart disease was observed.
There was no evidence to suggest increased mortality from cardiovascular disease, including arteriorsclerotic heart disease, among fire fighters in our study.
S021 - 1987
The overall standardised mortality ratio [for coronary artery disease] for fire fighters aged 45 to 54 years was 1.73 (P < .005).
Moreover, the confidence intervals for the overall age of 45 to 54 is such that the SMR is within the 95% confidence limits.
S013 - 1990
An increased mortality was seen for cancer and ischaemic heart disease but the differences did not reach statistical significance.
The results indicate that firefighting is associated with an increased risk of cancer. Also, they corroborate, to some extent the hypothesis that firefighting is associated with an increased risk of dying from ischaemic heart disease.
S003 - 1991
Heart disease ... occurred significantly less often than expected.
The significantly low [SMR] of 0.89 for death due to diseases of the heart was interesting in light of evidence that firefighters are exposed to carbon monoxide and other cardiovascular risk factors.
S009 - 1992
Mortality due to all causes, ischaemic heart disease ... was less than expected based upon United States rates for white men.
As anticipated, many of the results of this study are consistent with the healthy worker effect.
S014 - 1993
Mortality from all causes was close to the expected mortality ratio ... as was that for heart disease (1.10: 95% CI 9.2, 1.31), and neither was statistically significant.
Ischaemic heart disease ... and ... showed elevations (SMR 1.06), none of which ... attained statistical significance.
The major limitation of the present study is lack of power to demonstrate lower relative risks.
S007 - 1994
Ischaemic heart disease accounted for 289 deaths, of which 205 were due to actue myocardial infarction, with SMRs which do not vary substantially from 1.00.
There is conflicting evidence regarding the risk of cardiovascular disease among fire fighters ...
S008 - 1994
The mortality ... was lower than expected ... with a low mortality in circulatory diseases ...
The mortality from ischaemic heart diseases was close to the expected within all exposure groups.
S011 - 1995
None of the cause specific SMRs were significant different from unity.
It has been shown in this study that neither cancer nor cardiovascular mortality is significantly higher amongst firemen ...
These results could be questionable due to the number of observed deaths being too small for statistical power, and the short time period of the study.
S001 - 2001
For jobs with stringent physical fitness entry requirements, the lack of deficit of cardiovascular disease mortality in comparison to the general population is surprising and may indicate an absolute, albiet not relative, increased risk in ischaemic heart diseases.
S005 - 2001
There was no evidence that fire fighters were at an increased risk from any particular casue of death.
The overall mortality rate was lower than expected and the individual cause of death risks were not elevated.
A low mortality rate, due to the so-called "healthy worker effect", is expected in occupations, such as fire fighting, that require fitness and good health.
-
Study Year SMR P value Significance
ns = not significant
*=significantS006 1984 0.84 > 0.05 ns S027 1986 1.52 < 0.05 * S012 1987 0.92 > 0.05 ns S021 1987 1.73 < 0.05 * S013 1990 1.15 > 0.05 ns S003 1991 0.95 > 0.05 ns S009 1992 0.82 < 0.05 * S014 1993 1.06 > 0.05 ns S007 1994 1.04 > 0.05 ns S008 1994 0.98 > 0.05 ns S011 1995 0.74 > 0.05 ns S001 2001 1.09 < 0.05 * S005 2001 0.58 < 0.05 *
Definitions of variables in data file
| Column | Variable label | |
|---|---|---|
| Cause | Cause of death | |
| Study ID | Study number | |
| Type of estimate | MOR - Mortality odds ratio OR - Odds ratio PMR - Proportional mortality ratio RR - Rate ratio RLR - Relative risk SIR - Standardized incidence ratio SMR - Standardized mortality ratio | |
| observed | Reported number observed (* indicates not reported) | |
| expected | Reported number expected (* indicates not reported) | |
| Reported estimate | The estimate reported in the paper or report | |
| log(Reported estimate) | The natural log of the reported estimate | |
| Standard error | The standard error of the log(Reported estimate) | |
| Lower bound CI Upper bound CI | Bounds of a 95% confidence interval for the estimate. For mortality ratios exact confidence intervals are provided; for other estimates, reported confidence intervals or normal approximations are used. |
Glossary
Case-control study
A study that matches cases of a disease with disease-free controls to allow a comparison of the odds of exposure (e.g. being a firefighter).
Cohort study
A study that tracks a defined group or cohort of people over time to observe the rates of death or disease.
Epidemiology
The study of the causes and distribution of diseases in humans.
Healthy worker effect
A potential bias in comparisons of workers with the general population arising because the workforce generally includes healthy individuals whereas the general population includes individuals not well enough to work.
MFESB
Melbourne Fire and Emergency Services Board
Mortality odds ratio
The ratio of the odds of death for fire fighters relative to an appropriate reference population.
Odds ratio
The ratio of the odds of death (or disease) for fire fighters relative to an appropriate reference population.
Proportional mortality ratio
The ratio of the observed number of specific-cause deaths to the expected number of specific-cause deaths in a proportional mortality study; the expected number is based on applying the proportion of specific-cause to all-cause deaths from an appropriate reference population to the number of all-cause deaths in the study population.
Proportional mortality study
A study that observes the number of deaths in a study population (but not the person years).
Publication bias
A tendency to prefer to publish findings which are statistically significant (or have large effects) rather than results that are not statistically significant (or have small effects); it can reflect the preferences of researchers, reviewers and/or editors.
Rate ratio
The ratio of the rate of death (or disease) in the population of interest relative to the rate in a reference population.
Relative risk
The proportion of deaths (or disease) from a given cause in the population of interest relative to the same proportion in a reference population.
Standardized incidence ratio
The ratio of the observed number of cases of disease to the expected number of cases of disease in a cohort study; the expected number is based on an appropriate reference population.
Standardized mortality ratio
The ratio of the observed number of deaths to the expected number of deaths in a cohort study; the expected number is based on an appropriate reference population.
Epidemiological studies of fire-fighters included in the meta-analysis
-
This study is a large and important cohort study. It covered a long period of follow-up: 1925 to 1986, and had a large number of fire fighters enrolled: 7,789. The total person-years was 204,821. The outcome studied was mortality and SMRs were calculated using two reference populations: the general US population and the National Institute for Occupational Health and Safety Computerized Occupational Referent Population System (CORPS).
The study used a number of approaches to examining exposure measures using the proxies of career “runs”, company type (engine or ladder or both) and potential for diesel exposure. Latency analyses were carried out by lagging the exposure by ten years.
All cause and all cancer mortality was found to be similar to the US general population. Significantly low SMRs were found for several non-cancer outcomes, while significantly high SMRs were obtained for colon cancer (1.51) and ischaemic heart disease (1.09).
Baris D, Garrity TJ, Telles JL et al. Cohort mortality study of Philadelphia firefighters. American Journal of Industrial Medicine 2001; 39: 463-476.
-
Since 1984, several US agencies have supported the coding of industry and occupational title in many states. This study used these data to carry out a comparison of cancer mortality among fire fighters in 24 states between 1984 and 1993 with that of non fire fighters from the same population. Separate analyses were done for white and black male fire fighters. For all cancers combined the mortality odds ratio (MOR) was 1.1, and because of the large number of cases (1817), this was statistically significant. A number of specific cancers also showed excesses. A very large MOR of 6.9 (95% confidence interval: 3.0 to 16.0) was found for brain and central nervous system cancers among black fire fighters, based on 5 cases.
Ma F, Lee DJ, Fleming LE et al. Race-specific cancer mortality in US firefighters: 1984-1993. Journal of Occupational & Environmental Medicine 1998; 40: 1134-1138.
-
This was a cohort study of mortality among fire fighters in San Francisco, followed up between 1940 and 1982. There were 3,066 fire fighters and a total of 1,186 deaths. SMRs were calculated using the US general population as reference. All cause mortality and all cancer mortality was lower than expected; there were elevated SMRs for oesophageal cancer, cirrhosis and accidental falls.
Beaumont JJ, Chu GS, Jones JR et al. An epidemiologic study of cancer and other causes of mortality in San Francisco firefighters. American Journal of Industrial Medicine 1991; 19: 357-372.
-
This very large mortality cohort study followed fire fighters employed for more than three years in Boston since 1915. The follow-up period was 1/1/1915 to 1/7/1975. There were 5655 subjects, over 140,000 person-years and 2470 deaths. Expected numbers of deaths were calculated using both US and Massachusetts death rates.
SMRs were calculated for all and specific causes; the overall SMR was 91 and most were under 100; SMRs were also calculated separately for active and retired fire fighters.
Musk AW, Monson RR, Peters JM et al. Mortality among Boston firefighters, 1915--1975. British Journal of Industrial Medicine 1978; 35: 104-108.
-
This was a cohort study of mortality and cancer incidence. The background and motivation for the study was a cluster of four cases in Wellington between 1980 and 1991 of testicular cancer, regarded as unusually high. The United Fire Brigades Association of New Zealand maintains records for all New Zealand fire fighters in a registry. The follow up period of the study was 1977 to 1995. The cohort definition was that a study participant must have worked for a total period of at least one year in NZ as a paid fire fighter, and worked as a fire fighter at least one day between 1/1/77 and 30/6/95. Follow-up was to 31/12/95 for mortality, and to 31/12/96 for cancer incidence.
SMRs and SIRs for cancer were calculated using national data, with 5-year age and calendar periods, and sex. There were 4305 subjects: 4221 males and 84 females. There were 59,322 person-years for mortality and 63,057 for cancer incidence. 117 deaths and 118 cancers were observed. The SIR analysis was done on the males only.
Overall, there were no statistically significantly elevated SIRs. When the analysis was restricted to 1990 – 96 (due to greater confidence about the completeness of population registries for that period), the SIR for testicular cancer was statistically significantly elevated: 2.97 (95% CI: 1.3 – 5.9), based on 8 observed to 2.7 expected. Mortality was relatively very low overall: the all-cause SMR was 0.58.
Bates M, Fawcett F, Garrett N et al. Retrospective cohort study of mortality and cancer incidence in New Zealand fire fighters. 2000.
Bates MN, Fawcett J, Garrett N et al. Is testicular cancer an occupational disease of fire fighters? American Journal Industrial Medicine 2001; 40: 263-270.
-
This Australian mortality cohort study followed all men employed by the WA Fire Brigade between 1/10/1939 and 31/12/1978. There were 990 men, 16,876 person-years and 116 deaths. SMRs and SPMRs were calculated and reported; the expected numbers of deaths were based on WA rates. The authors concluded that there was “virtually no evidence in these data of an adverse effect of firefighting on mortality”.
Eliopulos E, Armstrong BK, Spickett JT et al. Mortality of fire fighters in Western Australia. British Journal of Industrial Medicine 1984; 41: 183-187.
-
This was a cohort study of mortality. The definition for cohort membership was: all employees who had worked in the six fire departments within metropolitan Toronto at any time between January 1, 1950 and December 31, 1989. Women and other exclusions lead to a cohort of 5414 men from the original 5995 for the primary analysis, among which 777 deaths occurred. For the analysis by length of employment there were data available from 5373 men, with 113,111 person-years of follow-up. SMRs were calculated by cause of death. Some analysis was carried out by years since first employment and years of first employment, and by age for selected causes.
Significant excesses were found for brain tumours, “other” malignant neoplasms, and aortic aneurysms.
Aronson KJ, Tomlinson GA, Smith L. Mortality among fire fighters in metropolitan Toronto. American Journal of Industrial Medicine 1994; 26: 89-101.
-
This cohort study examined both mortality and cancer incidence. The cohort definition was: all men who worked at least 1 year as a fire fighter in the City of Stockholm during 1931 – 1983. In the mortality analysis, there were 1116 men, 25,221 person-years and 316 deaths in the follow-up period for mortality, which was January 1, 1951 – December 31, 1986.
For the cancer incidence analysis, there were 1091 men, 21,049 person-years and 127 cancers in the follow-up period for incidence of January 1, 1958 – December 31, 1986. Some analyses were carried out by age, length of employment, latency (defined as years since first employment) and number of fires fought, the latter based on an index derived from a 10% sample.
Significant excesses were found for stomach cancer overall, and trends with exposure for stomach and brain cancer.
Tornling G, Gustavsson P, Hogstedt C. Mortality and cancer incidence in Stockholm fire fighters. American Journal of Industrial Medicine 1994; 25: 219-228.
-
This mortality cohort study was conducted in Seattle and Tacoma, Washington, and Portland, Oregon. It followed up 4546 fire fighters employed for at least one year between 1944 and 1989. Two reference populations were used: US national population white male death rates were used for determining SMRs, while a cohort of police from the same cities was used as a comparison for mortality rate ratios. There were 122,852 person-years of follow-up and 1169 deaths. Elevated SMRs for brain cancer and leukaemia were found; the former risk was more apparent in younger fire fighters while the latter risk was greatest among men with decades of employment.
Demers PA, Vaughan TL, Checkoway H et al. Cancer identification using a tumor registry versus death certificates in occupational cohort studies in the United States. American Journal of Epidemiology 1992;136:1232-1240.
-
This cohort study of cancer incidence was conducted in Melbourne, Victoria, and was based on 2,865 male fire fighters who had been employed by the Melbourne Fire Brigade between 1917 and 1989. The follow-up period was January 1, 1980 to December 31, 1989; there were 20,853 person-years and 50 cases of cancer. SIRs were calculated for various cancer sites and by time since first employment and duration of employment. None of these analyses showed a statistically significant SIR.
Giles G, Staples M, Berry J. Cancer incidence in Melbourne Metropolitan Fire Brigade members, 1980-1989. Health Reports 1993; 5: 33-38.
-
This was a cohort study of mortality, concentrating on cancer, in Paris, France. The cohort studies consisted of 830 male fire fighters of the Brigade des sapeurs-pompiers de Paris. They were followed up between 1977 and 1991. There were 11,414 person-years and 32 deaths. The all-cause SMR was 0.52 and the SMR for all neoplasms was 0.89. A number of the specific cancers had elevated SMRs but due to the small size of the study all of the corresponding confidence intervals included one.
Deschamps S, Momas I, Festy B. Mortality amongst Paris fire-fighters. European Journal of Epidemiology 1995; 11: 643-646.
-
This was a cohort study of the mortality of white male municipal workers in Buffalo, New York. Within the overall study there was a sub-study of the fire fighters of the workforce. The cohort definition required participants to have been employed for a minimum of five years for the City of Buffalo with at least one year as a fire fighter. The men were followed for the period between January 1, 1950 and October 1, 1979. There were 32,858 person-years and 470 deaths. SMRs were calculated for specific causes and a selection of cancer sites. Statistically significant excesses were observed for bladder cancer (SMR = 2.9) and colon cancer (SMR = 1.8). A number of analyses were carried out by various time-related measures.
Vena JE, Fiedler RC. Mortality of a municipal-worker cohort: IV. Fire fighters. American Journal of Industrial Medicine 1987; 11: 671 -684.
-
This cohort study compared cancer mortality in fire fighters with the same outcome in a group comprising other public employees in defined occupations, in Denmark. The membership of the cohort was determined by the occupations listed on the 1970 census. There were 886 fire fighters and 47,694 “unexposed” subjects; follow-up was between 1970 and 1980 and the groups contributed 8625 and 461,940 person-years respectively, a total of 470,565 person-years. There were 57 deaths among the fire fighters. Slightly elevated SMRs were found for all cancer, lung cancer and ischaemic heart disease; none of these was statistically significant.
Hansen ES. A cohort study on the mortality of firefighters. British Journal of Industrial Medicine 1990; 47: 805-809.
-
This was a cohort study of mortality. The cohort comprised all fire fighters employed between 1927 and 1987 by either of the fire departments of Edmonton or Calgary in Alberta, Canada. 3328 fire fighters were followed for 64,983.3 person-years; there were 370 known deaths. Cause-specific SMRs were analyzed, and there were also some analyses by latency, duration of employment and “exposure opportunity”.
The general conclusion was that there was very weak evidence for an excess risk among fire fighters for any particular cause.
Guidotti TL. Mortality of urban firefighters in Alberta, 1927-1987. American Journal of Industrial Medicine 1993; 23: 921-940.
-
This proportional mortality study compared numbers of deaths among fire fighters in New Jersey with the US general population, the New Jersey population, and a police population. The deaths were recorded through a comprehensive retirement system for police and fire fighters that exists in the state of New Jersey. 263 deaths among fire fighters were recorded between 1974 and 1980. The resulting PMRs varied according to the reference populations used. There were elevated PMRs found for heart disease, non-malignant respiratory disease and leukaemia, depending on the reference group used.
Feuer E, Rosenman K. Mortality in police and firefighters in New Jersey. American Journal of Industrial Medicine 1986; 9: 517-527.
-
This was a case-control study of brain cancers and employment. The exposure data was based on occupational history from hospital records at the time of diagnosis. Cases were white males diagnosed with histologically confirmed brain and other CNS cancers between January 1984 and 1988 in the Missouri Cancer Registry. Controls were frequency matched, chosen from all other white male patients diagnosed with cancer, excluding cancers of ill-defined or unknown sites. There were four controls per case. Based on 12 cases there was an excess among police and fire protection services, with an odds ratio of 2.2; the OR for fire fighters specifically was greater than 2, but not statistically significant.
Brownson RC, Reif JS, Chang JC et al. An analysis of occupational risks for brain cancer. American Journal of Public Health 1990; 80: 169-172.
-
This cohort study followed men employed as fire fighters in Toronto, Ontario, who were employed between 1/4/1918 to 1/4/1954. Over 1800 firemen were enrolled. Deaths were observed over the period 1921 to 1953, and 25,918 person-years accrued.
Comparison with Ontario men showed both a significant excess (cardiovascular-renal) and deficits (respiratory, tuberculosis). Comparison with Toronto men was restricted to 1937 – 53 and showed a similar pattern, but a significant excess for all causes: O=203, E=171.
Mastromatteo E. Mortality in city firemen II. A study of mortality in firemen of a city fire department. AMA Archives of Industrial Health 1959; 20: 55-61.
-
This case-control study used cases from the Massachusetts Cancer Registry (MCR) for 1982 – 86; nine different cancer types were analyzed. Controls were apparently also from MCR. Exposure was either defined only among those who were fire fighters or police, or among all males. Significantly high ORs were found for several cancers, depending on which group was used (police or state).
Sama SR, Martin TR, Davis LK et al. Cancer incidence among Massachusetts firefighters, 1982-1986. American Journal of Industrial Medicine 1990; 18: 47-54.
-
This study looked at a cohort of subjects enrolled in a study of aging in Boston, Massachusetts known as the Normative Aging Study. There were 171 fire fighters and 1475 non fire fighters who had three complete medical examinations, approximately 5 years apart, or a diagnosis of coronary heart disease (including death from CHD) by the third examination. The rate ratio for CHD among the fire fighters was 0.5, although there were only 4 cases and this rate ratio was not statistically significant.
Dibbs E, Thomas HE, Weiss ST et al. Fire fighter and coronary heart disease. Circulation 1982; 65: 943-946.
-
This case control study used occupation as listed on death certificates. 904 deaths from brain tumours between 1969 and 1978 in Washington, USA were analysed; controls were randomly chosen from other deaths, excluding leukaemia. The odds ratio for “fire fighting/prevention occupations” was 1.3, with a 95% confidence interval of 0.5 to 3.9.
Demers PA, Vaughan TL, Schommer RR. Occupation, socioeconomic status, and brain tumor mortality: a death certificate-based case-control study. Journal of Occupational Medicine 1991; 33: 1001-1006.
-
This study examined deaths rates from coronary artery disease in a cohort of fire fighters employed for at least 6 years in the Toronto Fire Department. The cohort was aged between 45 and 54 and was followed up between 1970 and 1983; there were 596 men who contributed a total of 4,142 person-years. SMRs were calculated using rates from the city of Toronto. The SMR for coronary heart disease was 1.73, with a 95% confidence interval of 1.12 to 2.66.
In the statistical results of Bates (1987) there are several anomalies. Notably, the overall SMR of 1.73 is not equal to the ratio of the overall observed to the overall expected (21/10.92 = 1.92). On closer inspection, there are related discrepancies between the observed and expected values and the SMRs in several instances. A conservative approach was adopted, of taking as correct the published SMR (this being the lower of the two alternatives) and the published number of deaths.
Bates JT. Coronary artery disease deaths in the Toronto Fire Department. Journal of Occupational Medicine 1987; 29: 132-135.
-
This proportional mortality study examined deaths across 27 states in the USA, from 1984 – 1990, using the National Occupational Mortality Surveillance database. There were 5744 deaths in fire fighters. There were several significantly high PMRs, including all cancers (1.10), and fire-related accidents (2.42).
Burnett CA, Halperin W, Lalich N et al. Mortality among fire fighters: a 27 state survey. American Journal of Industrial Medicine 1994; 26: 831-833.
-
This study followed the cancer incidence experience of 2,447 fire fighters from two northwestern US cities between 1974 and 1989. Population based cancer registries were established in these cities in 1974. The cancer rates were compared with the local population rates and also with those found in a cohort of 1,878 policemen from the same two cities. 35,083 person-years of follow-up were achieved; there were 224 cases of cancer. There were a number of elevated SIRs, but these were mostly based on small numbers and were not statistically significant. The main exception was prostate cancer, for which the SIR of 1.4 had a 95% confidence interval of 1.1 to 1.7. This and other SIRs which used the general population as reference were generally reduced when the police cohort was used to find a rate ratio.
The study examined cancer rates by length of employment and by time since first employment. Overall the authors concluded that the study did not find strong evidence for an excess risk of cancer.
Demers PA, Checkoway H, Vaughan TL et al. Cancer incidence among firefighters in Seattle and Tacoma, Washington (United States). Cancer Causes & Control 1994; 5: 129-135.
-
This study monitored a 10% sample of the Canadian labor force by computerized record linkage to the Canadian mortality statistics. The follow-up period was between 1965 and 1979, during which 1006 men who worked at least one year as a fire fighter between 1965 and 1969 were found to have 26 cancer deaths. The reference population used to calculate expected numbers of deaths was the whole cohort, and therefore consisted of employed individuals. The multiple myeloma SMR was 10, which was statistically significant even though only based on 2 cases.
The general report for this study is in the paper by Howe and Lindsey (1983). That paper does not include results for fire fighters. However, in the review paper on fire fighters and the risk of cancer by Howe and Burch (1990), reference is made to results from the labor force data, with a citing of Howe and Lindsey (personal communication). We are not aware that the results have been published elsewhere in a more substantive manner.
Howe GR, Burch JD. Fire fighters and risk of cancer: an assessment and overview of the epidemiologic evidence. American Journal of Epidemiology 1990; 132: 1039-1050.
-
This PMR study considered the 1969 to 1988 mortality experience of male fire fighters with at least one year of service in the City of Honolulu Fire Department, Hawaii, USA; the reference was the male Hawaiian population. 205 fire fighter deaths were included. A significantly low PMR of 0.37 was found for lung diseases; elevated PMRs were obtained for cirrhosis of the liver (2.30), prostate cancer (2.61) and brain cancer (3.78, 95% confidence interval 1.22 to 11.71, based on 3 deaths), as well as some general outcomes: genitourinary system cancer (2.28) and all diseases of the circulatory system (1.16) Separate analyses were carried out for Caucasian and Hawaiian fire fighters.
Grimes G, Hirsch D, Borgeson D. Risk of death among Honolulu fire fighters. Hawaii Medical Journal 1991; 50: 82-85.
-
This study followed 5,568 fire fighters from five brigades in the UK over a period of 30 years. Mortality and cancer incidence were recorded. SMRs were calculated using two reference populations: England and Wales, and a comparable cohort from the Office of Population Censuses and Surveys Longitudinal Study. SIRs were found using cancer rates from England and Wales.
All SMRs and SIRs were below one; several were statistically significant.
The only report found of this study was on a website, and was an Issue of the “Fire Research News” from the Fire Research and Development Group, Office of the Deputy Prime Minister. If this indeed the only publication from this study, it is rather striking that such a large study appears not to have been published in any academic journal, or even as a formal report.
Direct correspondence was attempted with the researcher stated to be responsible for the study, Professor Stuart Donnan. No contact was established, and his successor at Manchester University was not able to shed light on this study.
For these reasons the results from this study should be treated with caution, as they have apparently not been subject to any academic peer review.
Gooderson C. A summary of a thirty year study of mortality in firefighters in Great Britain. Office of the Deputy Prime Minister, Fire research and development group, Fire Research News, Issue 21, Winter 1997. [Internet source: http://www.safety.odpm.gov.uk/fire/fepd/frp/frn/frn21/01.htm]
-
This study’s primary data source was death certificates from the State of Connecticut between the years 1960 – 1978. SMRs and mortality odds ratios were calculated, comparing the deaths from ischaemic heart disease (IHD) among fire fighters with the male working population of Connecticut during the same period (SMRs), and with the whole population (MORs). A direct comparison was also made with policemen. There were 115 IHD deaths among firemen. The SMR for ischaemic heart disease was 1.52; 95% confidence interval: (1.23 to 1.81). The MOR was 1.07 (0.91 to 1.23) and the MOR in relation to police was 0.62 (0.56 to 0.68).
Sardinas A, Miller JW, Hansen H. Ischemic heart disease mortality of firemen and policemen. American Journal of Public Health 1986; 76: 1140-1141.
-
This study was reported in a publication of the California Department of Health Services. We have been unable to obtain a copy of the report, and are therefore relying on the results of the study as presented in Table 1 of the review of Guidotti (1995). While these are brief, they do indicate some of the features of the study and its outcomes. It was a mortality cohort study. SMRs were calculated in the usual fashion, and also “adjusted for presumed rates of smoking, alcohol intake and socio-economic status”. Without the original report, it is not possible to assess the nature of this adjustment. It is these adjusted SMRs that have been used in the current report; in almost all cases, they were lower than the unadjusted SMRs.
The size of the study and the follow-up period are not specified in Guidotti’s review.
The results in Guidotti’s Table 1 are in the form of SMRs and 95% confidence intervals, without observed and expected numbers of deaths. By investigating possible methods for calculating confidence intervals, it became apparent that the exact method had been used, and it was therefore possible to obtain the observed and expected values corresponding to the results. This made possible the incorporation of this study into the general synthesis of studies.
California Department of Health Services. California Occupational Mortality, 1979-1981. Health Demographics Section. 1987.
-
This study was reported in an abstract from the conference of the Society for Epidemiologic Research. It was a PMR study in Florida USA, involving 1,411 deaths among fire fighters between 1972 and 1999. There were 364 deaths due to malignant neoplasms. Significant excess mortality was observed for all cancer combined (PMR = 1.13), respiratory cancer (1.23) and skin cancer (2.35). The PMR for prostate cancer was significantly low (0.57).
As was the case for study S028, described above, the results were provided in the form of PMRs and 95% confidence intervals, without observed numbers (apart from the overall numbers of deaths and cancer cases). Again, investigation of possible methods for calculating confidence intervals revealed that the square root transformation with a normal approximation was used, and it was therefore possible to obtain the observed and expected values corresponding to the results. Thus the results available from this study were also able to be incorporated into the synthesis of studies.
Ma F, Fleming LE, Lee D et al. Cancer mortality among Florida firefighters. American Journal of Epidemiology 2002; 155(Suppl): 312-312.
-
This was a very detailed study of male white deaths in the state of Massachusetts between 1971 and 1973. Standardised mortality odds ratios for all cancers were obtained for every occupation and for cirrhosis of the liver; the method used was essentially a case-control approach, in which the cancer of interest provided all the cases, and the deaths from other causes served as the controls. Each occupation, in turn, constituted the exposed group. Results were presented adjusted for age alone, and for age and social class; the results included here are the latter.
There were 129 cancers and 16 deaths from cirrhosis of the liver. The SMORs reported in Table 1 of Guidotti (1995) are not available in the hard copy of Dubrow and Wegman; they were located in a comprehensive listing of all cancers and occupations on a set of microfiche accompanying the report. Because the SMOR is a different measure to the SMR, and only close to it for relatively large numbers, the observed and expected numbers from the microfiche were only recorded for review in this report if the smaller of the two was at least four.
Most of the SMORs were smaller than 1. The all cancer mortality odds ratio was 0.82, and a significantly low SMOR for prostate was observed.
Dubrow R, Wegman DH. Occupational characteristics of cancer victims in Massachusetts, 1971-73. Cincinnati OH, NIOSH Research Report, 1984.