Preventing falls
Introduction
Falls are one of the major causes of admission to hospital for elderly people. Falls in the elderly can result from deteriorating physical health and fitness, failing vision and hazards around the home. Preventing falls in the elderly has enormous health, social and economic benefits. In Victoria, the annual cost of falls is estimated to be over $500 million. This study examined three interventions designed to reduce the risk of falling – exercise, vision correction and removal of home hazards – alone and in combination.
The study was a collaboration between The City of Whitehorse, Dr. Lesley Day, Dr. Brian Fildes and Michael Fitzharris (researchers from the Monash University Accident Research Centre), Dr. Harold Flamer (a geriatrician from the Peter James Centre), Dr. Stephen Lord (a researcher from Prince of Wales Medical Research Institute, Sydney) and Dr. Ian Gordon (a statistician from the Statistical Consulting Centre at The University of Melbourne).
The key question that the study team wanted to answer was:
Which intervention or combination of interventions best reduces the risk of falls in elderly people living at home?
Timeline
- 1993
-
Whitehorse Council asked Monash University Accident Research Centre to implement a falls prevention program.
Commonwealth Department of Health, Housing, Local Government and Community Services approves a feasibility study of a falls prevention program.
- Early 1994
-
Proposal for falls prevention study to Commonwealth Government
- 1994
-
Ethics approval obtained from Monash University standing committee on ethics in research involving humans.
- April 1995
-
City of Whitehorse approved community-based study.
- 1995
-
Study design finalised
Falls program co-ordinator appointed
Home assessors recruited and trained - January 1996
-
Data collection commenced
- July 1999
-
Data collection completed
- 1999-2000
- 2001
-
Report produced
- 2002
-
“Randomised factorial trial of falls prevention among older people living in their homes” appears in the British Medical Journal.
- Today
Background
Falls in the Elderly
In many countries, including Australia, injuries due to falls are one of the most common reasons for hospital admission in the elderly. Elderly people are at a higher risk of falling than younger adults. Elderly people often suffer more serious problems as a result of falls than younger adults. These problems include reduced mobility, increased dependence on mobility aids and an inability to live independently at home. Psychological problems can also result, including increased anxiety, loss of confidence and withdrawal from social activities.
Elderly people are susceptible to falls for a variety of reasons. Factors relating to aging include the increased incidence of medical problems such as stroke and arthritis, deteriorating balance, difficulty walking, and the increased use of medicines, including sedatives. Environmental factors include stairs that are difficult to negotiate or in poor condition, poor lighting, slippery floors, slippery mats and rugs, and slippery surfaces in bathrooms.
The consequences of falls are often worse for the elderly due to their more brittle bones. The injury sustained from a fall is related to the extent of brittleness in an individual’s bones.
Several types of interventions aimed at reducing the risk of injury in the elderly have been tried in Australia and overseas. These include education programs, home modifications, behaviour change and exercise. Some of these interventions were evaluated. However, there were problems with the evaluations, including small sample sizes, lack of a control group, failure to control for baseline differences between control and intervention groups, and reliance on participants’ recall of falls over a long period of time.
Objectives
The primary objective was to investigate the effectiveness of three interventions – exercise, vision correction and home hazard removal – for reducing fall risk in elderly people living at home. The study design allowed examination of the effects of the interventions alone and in combination.
A second objective was to explore the effects of the interventions on other factors related to falling. These included psychological factors like fear of falling, and health-related factors such as use of medical services.
Interventions
The exercise intervention involved attending 15 weekly strength and balance exercise sessions led by trained instructors. Participants were asked to do 30 minutes of the exercises at home every day.
Participants receiving the vision correction intervention were referred to eye specialists for problems identified in the baseline risk assessment.
The home hazards removal intervention involved removal of home hazards identified in the baseline risk assessment subject to the agreement of the participant and provided that the work required was not costly.
Summary of stages in the study
- Recruitment letter sent to all residents aged 70+ in the City of Whitehorse
- Telephone follow-up of those not responding to the recruitment letter
- Telephone screening for initial inclusion and exclusion criteria
- Home-based baseline assessment of background and risk factors
- Random assignment to the intervention group
- Appropriate intervention(s) implemented
- Ongoing recording of falls by participants
- Falls calendars are mailed each month
- Follow-up of participants failing to return the calendar
- Random selection of participants for follow-up assessment
- Home-based follow-up assessment of risk factors
Funding
The project was funded by the National Health & Medical Research Council, the Victorian Department of Human Services (Aged Care), the City of Whitehorse, the Victorian Health Promotion Foundation, and the National Safety Council.
Study design
Ethics
Hear discussion with Lesley Day about potential ethical issues in both designing and conducting the study by watching the video.
Variables
-
- Age
- Gender
- Marital status
- Living alone (yes or no)
- Post high school education
- Fall in the last month (yes or no)
- Activities of daily living
- Use of support services
- Falls efficacy scale
- Number of medications taken
-
- Quadriceps strength (left and right)
- Postural sway in bare feet
- Postural sway on foam mat
- Maximal balance range
- Number of errors on dynamic balance test
- Timed-up-and-go test (time to complete test)
- Single leg balance (left and right)
- Low contrast acuity (left and right eye)
- High contrast acuity (left and right eye)
- Presence of stereopsis
- Field of view
- Total number of home hazards
- Height (cms)
- Weight (kg)
-
- Exercise intervention
- Vision intervention
- Home hazard intervention
-
- Self-reported falls (time to nth fall)
A fall was an accident where balance was lost and part or all of the body hit the ground.
Structured telephone interview:
- Circumstances of fall
- Details of what happened during the fall
- Injuries from fall
- Care sought as a result of the fall
-
- Activities of daily living
- Use of support services
- Falls efficacy scale
- Number of medications taken
- General practitioner visits
- Hospital admissions
- Quadriceps strength (left and right)
- Postural sway in bare feet
- Postural sway on foam mat
- Maximal balance range
- Number of errors on dynamic balance test
- Timed-up-and-go test (time to complete test)
- Single leg balance (left and right)
- Low contrast acuity (left and right eye)
- High contrast acuity (left and right eye)
- Presence of stereopsis
- Field of view
- Total number of home hazards
Statistician’s description of the design
The study was a randomised controlled trial that examined the effectiveness of three interventions in reducing falls among the elderly.
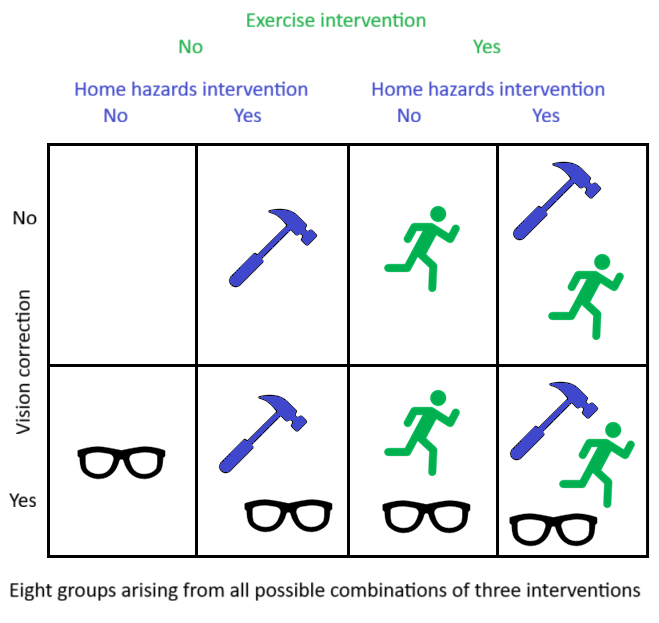
It was a full factorial design with three factors – exercise, vision improvement and home hazard reduction – each with two levels. Hence, the trial included 8 independent groups.
Computer software was used to assign each participant randomly to one of the eight groups.
Planning of the trial involved estimating the number of participants required, described further below.
Calculating the sample size for the study
An estimate of the sample size needed was calculated in the following way:
- The annual rate of falls if there was no intervention was assumed to be 35 falls / 100 people. This figure was based on recent data.
- It was assumed that any one intervention alone would reduce the rate of falls by 25%. Therefore, for the intervention group, the rate of falls would be 26 falls / 100 people.
- It was assumed that there is interest in detecting both positive and negative changes in the intervention group. Sample size calculations were based on a two-sided test.
- The significance level was set at 5%.
- The power – the probability of detecting a true difference between the control and intervention group – was set at 0.80.
- Using the assumptions above, 914 participants were required.
- It was assumed that 20% of those who initially agreed to participate would drop out.
- Hence, the final sample size required is 1143, since 914 = 80% of 1143.
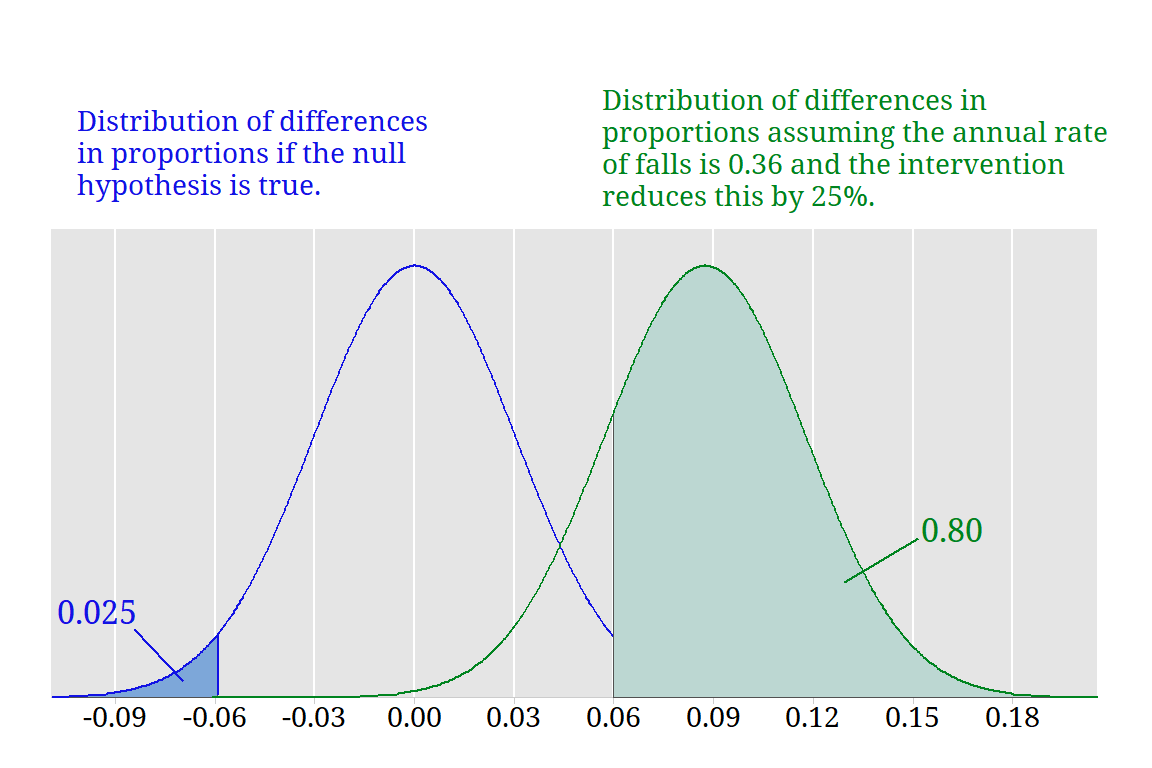
The figure shows sampling distributions of the difference in proportions between the control and intervention group with equal sample sizes of 457. The blue distribution is the sampling distribution when the true proportions in the experimental and control groups are equal. The green distribution is the sampling distribution of differences in proportion when the intervention reduces the annual rate by 25%.
Randomisation procedure
As participants were recruited into the study, they were randomly assigned to one of the eight treatment groups. Hence, entry to the study was “staggered” and there was potential for imbalance in the number of participants assigned to the eight groups. This is particularly a problem if the number of participants is small.
The randomisation procedure used attempted to adjust for this potential imbalance. The computer software used produced randomisation charts following an adaptive biased coin procedure. The adaptive biased coin procedure adjusts the probability of assignment to group i at any given time according to the degree of imbalance in the current group assignments, giving slightly higher probabilities of allocation to groups with disproportionately low numbers.
Sample randomisation chart
| Number of treatment groups | 8 |
|---|---|
| Total number of subjects | 60 |
| This chart commenced at subject number | 46 |
| Treatment | Previous tally | Cumulative tally in this chart |
|---|---|---|
| Control | 5 | 7 |
| Home modification | 6 | 8 |
| Exercise | 5 | 7 |
| Vision | 5 | 7 |
| Home modifications and Exercise | 6 | 7 |
| Home modifications and vision | 6 | 8 |
| Exercise and vision | 6 | 7 |
| Home modifications, exercise and vision | 6 | 9 |
References on the randomisation procedure
Lachin, J.M. (1988) Statistical properties of randomization in clinical trials. Controlled Clinical Trials, 9, 289-311.
Wei, L.J. (1978) The adaptive biased-coin design for sequential experiments. Annals of Statistics, 6, 92-100.
Wei, L.J. & Lachin, J.M. (1988) Properties of urn randomization in clinical trials. Controlled Clinical Trials, 9, 345-364.
Data collection
-
Advertisements Local papers, community radio, channel 31 Posters & brochures (multilingual) Service and Probus clubs, Neighborhood houses, Community centres, Home care, Meals on wheels Presentations Senior citizens organisations, Social clubs Displays Shopping centres Personal contact General practitioners, Physiotherapists, Hospital staff Participant recruitment Sampling frame Identify all people over 70 years old listed on the Australian Electoral Roll in the City of Whitehorse. Recruitment Send recruitment letter to all those identified as eligible from the Electoral Roll. Non-respondents are followed up with a telephone call to explain the study and invite them to participate.
-
Initial screening Ask potential participants initial screening questions on first telephone contact. Inclusion criterion Potential participants should be living in own home or in rented accommodation where home hazards could be modified. Participation in the study is approved by the potential participant’s general practitioner.
Exclusion criteria Exclude any potential participant who: - has a partner living in same home already in the study
- anticipates moving from the area within two years
- has participated in an exercise program similar to the exercise intervention in the last 2 months
- cannot walk 10-20 metres without rest
- cannot walk 10-20 metres without assistance
- cannot walk 10-20 metres without experiencing angina
- has respiratory disease
- has cardiac disease
- had psychiatric illness that prevents participation in interventions
- has dysphasia (a speech impairment)
- has recent modifications to home
- fails the Short Portable Mental Status Questionnaire (a measure of organic brain problems)
-
Assessors A trained assessor makes a home visit to collect background information and assess risk factors. The assessor does not know which intervention(s) the participant will receive, because the random allocation to treatment group has not yet occurred. Questionnaire Home assessor interviews participant to complete background and risk factor questionnaires. Measures include a Falls Efficacy Scale which gives a quantitative measure of the fear of falling during activities of daily living. -
Quadriceps strength Participant should be seated. Attach spring gauge to one ankle. Record quadriceps strength in kilograms while leg is extended. Repeat three times, and record the best result. Repeat the procedure for the other leg. Postural sway Measure postural sway using the Lord swaymeter under two conditions: (i) in bare feet, and (ii) standing on 8.5cm thick foam pad. Attach the swaymeter belt to the participant’s waist. The rod connected to the belt should be behind the participant. The belt is connected by the rod to a pen. Ensure that the pen and graph paper are placed on a stable surface. The participant’s body movement should be traced on the graph paper by the pen. Maximal balance range Again use the Lord swaymeter with the rod behind the participant. Ask the participant to lean backwards and forwards. The participant should attempt to go as far as possible without losing balance. The test should be attempted three times and the best result recorded. Record the distance travelled by the swaymeter pen for the best attempt. Dynamic balance Use the Lord swaymeter with the rod in front of the participant. Show the participant the pattern to be traced on the swaymeter graph paper. The participant should keep both feet on the ground while moving his or her body to follow the pattern. Record the number of times the pen moves outside the track to be traced, and add 5 every time a corner is cut. Timed-up-and-go test Seat the participant in a chair without arm rests. Ask the participant to get up from the chair, walk three metres, turn around, walk back to the chair and sit down. Record the time taken in seconds. Single leg balance The participant should remove his or her shoes. Ask the participant to balance on one leg without any supports for one minute. Record the time in seconds that the participant is able to balance on one leg. Repeat for the other leg. Height Measure participant’s height (shoes removed) in cm. Weight Measure participant’s weight in kg. Visual acuity: Conduct visual acuity tests in the best lit room in the participant’s home. Open all curtains and turn on all lights. Low & high contrast charts Seat participant two metres from test charts. First use low contrast version of standard letter chart. Cover one eye and ask participant to read chart starting from the line with the largest letters. Record the smallest line the participant could read correctly (entirely or in part). Repeat for other eye. Second use high contrast version of standard letter chart and repeat the test. Random dot stereo butterfly chart 1. Ask participant to identify (butterfly) pattern in random dots. 2. Present participant with depth discrimination cards, one at a time, from easiest to most difficult. Each depth discrimination card shows four circles. Ask the participant if any circle on the card appears to be forward from the other circles. (Every card includes one circle that appears forward from the others.) Continue until the participant gets one card wrong. Record the number of correct cards.
OKP glaucoma screening test Present participants with the test chart; it shows a series of numbers in a spiral pattern with a black spot in the centre. Cover one eye and ask the participant to read each number and indicate if the black spot disappears. Record the number of times the black spot disappears. Repeat for the other eye. (This is a test of field of view.) Home hazards Examine the rooms used in a normal week by the participant and record the hazards identified. -
Once the questionnaire and risk assessment are completed, participants should be randomly assigned to one of the eight groups. The random assignment is undertaken using a software program administered by a person not otherwise involved in the conduct of the study.
-
Exercise intervention Fifteen weekly 35-55 minute strength and balance exercise class led by VicFit instructors. Daily 25-30 minute home-based strength and balance exercises. Vision intervention Untreated visual problems identified in baseline assessment are referred to a general practitioner, optometrist or other eye specialist as appropriate. Home hazard intervention Removal of home hazards identified in baseline assessment. Participant agreement is required to remove any hazard. Hazard may be removed by participants or by the Council Home Maintenance program (up to a cost of $100). Combined interventions Participants assigned to combined intervention groups should receive all relevant interventions. No intervention Participants assigned to the “control” group did not receive any of the interventions during the study period. They were offerred an intervention after the study was finished. -
Follow-up period 18 months Falls calendar Each day, participants record, on a “Falls calendar”, whether or not they have fallen. At the end of each month, participants return the calendar by reply-paid post. Calendar follow-up Research assistant telephones participants who have not returned monthly calendars 10 working days after the end of the month. Falls interview Research assistant conducts structured telephone interview with participants who report having fallen to obtain details about the fall. Follow-up assessment Timing Follow-up assessments at 18 months were undertaken for half the participants. Random selection Randomly select 1 in 2 participants for follow-up assessments. Assessment Repeat the risk factor assessments made at the baseline assessment. The assessor should not know which intervention(s) any participant has received.
About the calendars
“Do you think the study was different from what it otherwise might have been because you got a statistician involved?”
Summary
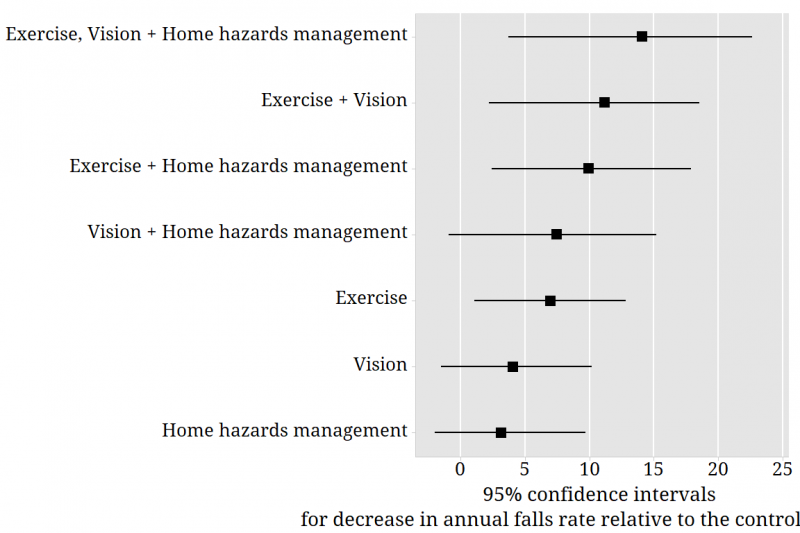
One thousand and ninety people aged 70 years or more and living at home participated in the study. The researchers summed up their findings in the British Medical Journal: A weekly exercise program focusing on balance, plus exercise at home, can help to prevent falls among Australians aged 70 years and over living at home and in good health. Home hazard management and vision screening and referral are not markedly effective in reducing falls when used alone but add value when combined with the exercise program.
Definitions of variables in data file
The data provided here is not the original data. The commitment given to study participants does not permit release of individual records. A data set has been generated with properties that are very similar to those in the original study.
| Subject | Participant number | |
|---|---|---|
| Group | 1 | Exercise, vision and home hazards interventions |
| 2 | No interventions (control group) | |
| 3 | Exercise and vision interventions | |
| 4 | Home hazards intervention | |
| 5 | Exercise and home hazards interventions | |
| 6 | Vision and home hazards interventions | |
| 7 | Vision intervention | |
| 8 | Exercise intervention | |
| Exercise | 0 = No exercise intervention, 1 = Exercise intervention | |
| Vision | 0 = No vision intervention, 1 = Vision intervention | |
| Home hazards | 0 = No home hazards intervention, 1 = Home hazards intervention | |
| Time | Time to first fall in days | |
| Censoring | 0 = Censored, 1 = Not censored (participant has had a fall) | |